

Published Sep 16, 2020
9 minute read

There are two major categories of breast reconstruction: implant based reconstruction, and reconstruction using your own tissue (known as autologous reconstruction). In some cases, a combination of techniques using your own tissue combined with an implant may be offered. Each technique has a different length of surgery, recovery time, advantages and disadvantages.
Implant reconstruction is often simpler and faster than autologous reconstruction. Using an implant avoids additional surgery in a donor area and for this reason often results in a faster recovery. On the other hand, implants do not last forever and will often need to be adjusted or replaced at some point in the future.
Implants have significantly higher complication rates in the setting of radiotherapy. If your treatment has included or will include radiation therapy, your surgeon will discuss whether implant reconstruction is still a good option for you.
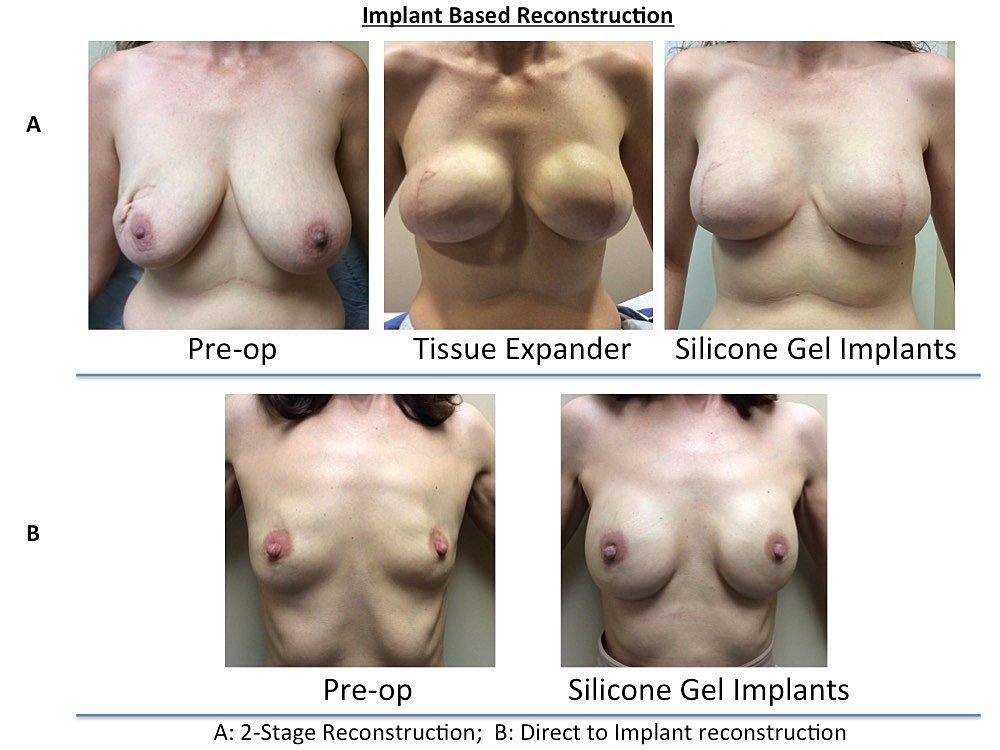
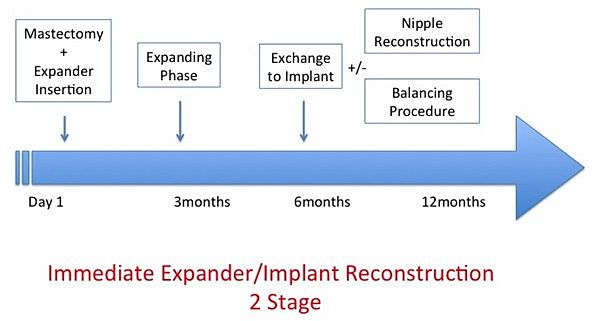
This staged method of reconstruction involves stretching the breast skin and tissue over a period of time prior to insertion of the final implant.
During the first stage, a temporary inflatable implant called a tissue expander is placed under the skin and muscle to stretch the tissues and allow for the creation of a breast mound. The expander is inflated in the clinic every 2 weeks over 2-3 months, using saline.
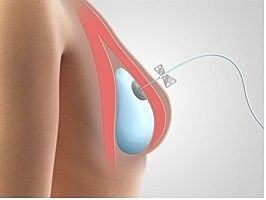 Tissue expander in place under the skin and muscle of the mastectomy site. It is filled by a small needle placed through the skin at each clinic visit.
Tissue expander in place under the skin and muscle of the mastectomy site. It is filled by a small needle placed through the skin at each clinic visit.
The second stage is carried out 3-6 months after the final expansion. The temporary expander is removed, and breast implants are inserted. Silicone implants are almost always recommended for use as the permanent implant in breast reconstruction. Silicone implants are completely safe and provide a more natural look and feel. Saline implants are heavier and tend to result in a more unnatural look and feel of the breast.
Each of these stages involves a 2-hour surgery under general anesthetic but does not usually require an overnight stay in the hospital. Recovery after the first stage lasts 2-4 weeks, and after the second stage lasts 1-2 weeks.
In certain cases, the permanent silicone implant can be placed at the time of mastectomy without the need for a tissue expander stage. Typically, a specialized material made from donated skin, known as acellular dermal matrix, must be used to further support the internal lining of the breast. Direct-to-implant reconstruction completes the majority of the reconstruction in one stage (2-3 hours) at the same time as the mastectomy. Often a second, smaller surgery is needed several months later to make minor adjustments or refinements. This type of reconstruction does not usually require an overnight stay in hospital.
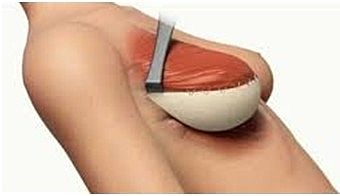 Acellular Dermal Matrix (beige) is used together with the Pectoralis muscle (red) to fully cover and support the implant under the breast skin.
Acellular Dermal Matrix (beige) is used together with the Pectoralis muscle (red) to fully cover and support the implant under the breast skin.
Using your own tissue can result in a more natural feeling and appearing breast. Since this is your own tissue, it will age and change with the rest of your body, often with less need for revisionary surgery in the future. On the other hand, autologous reconstruction necessitates additional, often complicated, surgery at the donor site (abdomen or elsewhere). This can result in longer healing and recovery times, and potentially a higher rate of short-term complications.
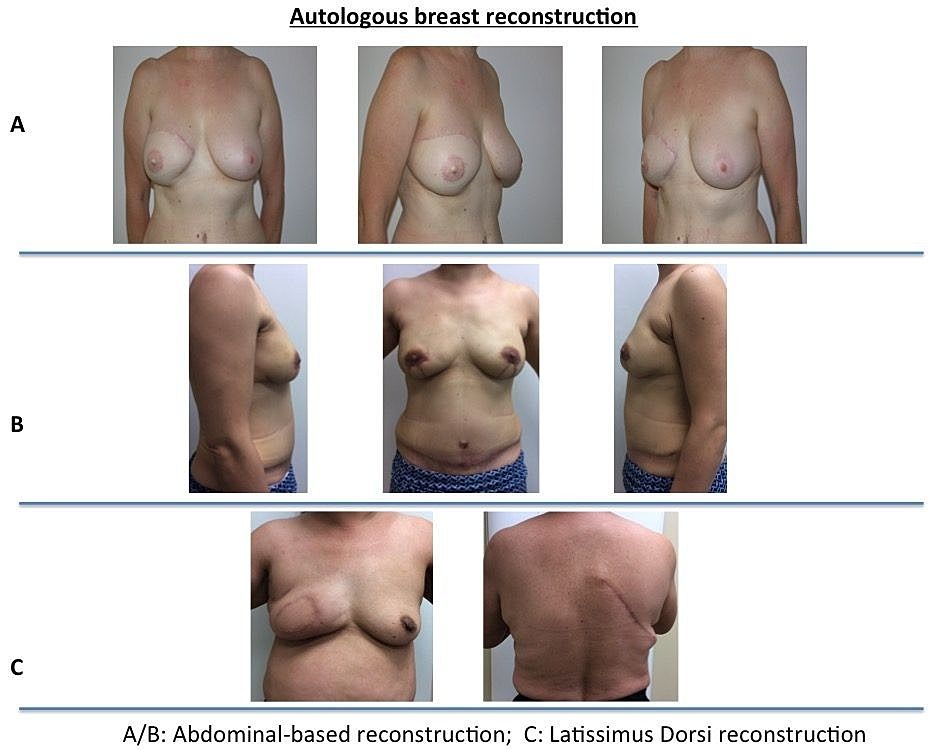
When reconstruction is performed with a Pedicled TRAM flap, the skin and fat of the lower abdomen remains connected to its blood supply via the underlying abdominal muscle (rectus abdominis). The muscle is transected at its lowermost point near the pelvis and rotated upwards into the chest area, where the attached skin and fat are used to create a breast mound. In this manner, the abdominal muscle is sacrificed from its native position in the abdomen and transferred to the chest, leaving a small amount of weakness and a higher chance of abdominal hernia or bulge in the future. This is a 3-ReplaceAddressLinkay in hospital.
A second option, also using abdominal tissue, is the Deep Inferior Epigastric Artery Perforator (DIEP) flap. This is known as a ‘free flap’ procedure, as it involves disconnecting skin and fat entirely and reconnecting it in the chest for breast reconstruction. The DIEP flap uses the same abdominal skin and fat as the TRAM flap but in a significantly more complicated way. Unlike the pedicled TRAM flap which remains attached to its blood supply, thereby sacrificing the abdominal muscle that is placed up in the chest, the DIEP flap uses microsurgical techniques to disconnect the skin and fat from its blood supply in the abdomen and reconnect it to a new blood supply in the breast area.
This procedure has the advantage of leaving the abdominal muscle intact, thereby decreasing abdominal weakness and lowering the risk of hernia that can sometimes be a problem with the pedicled TRAM flap. On the other hand, the DIEP involves a significantly longer and more complicated surgery (5-7 hours per side) with a small chance (1-3%) that the reconnected blood vessels do not flow properly. The DIEP procedure also requires a longer hospital stay (3-4 days) to allow for close monitoring of the flap.
There are a number of other free flap options that involve disconnecting skin and fat from various body areas and reconnecting them in the chest to create a breast mound. These procedures are not commonly performed but include flaps of tissue from the buttock (gluteal free flap) or the inner thigh (transverse upper gracilis). These flaps are rarely the first choice, but your surgeon can discuss these options with you if they may be appropriate.
In some cases, such as in the setting of previous radiation therapy, implant reconstruction may be considered in combination with using your own tissue from your back. The first stage of this surgery takes 3 hours and requires an overnight stay in hospital. During this surgery, the latissimus dorsi muscle from your back is transferred to your chest – often a variable amount of skin and fat from the back is transferred together with the muscle. This muscle harvest requires a long incision on the back, which is placed so that it will be hidden by clothing or a bra.
Once the muscle has been transferred to the chest, if additional volume/size is required, a tissue expander or implant can be placed beneath the latissimus dorsi muscle. Recovery time is 4-6 weeks following a latissimus dorsi flap. If an expander needs to be exchanged for a permanent implant, this is done during a secondary operation. This exchange operation is 1-2 hours long and requires 1-2 weeks of recovery.
Our goal is for you to have natural looking, symmetrical and aesthetically pleasing breasts following your breast cancer surgery. In some cases, small “touch up” procedures are required to make adjustments to the shape of the breasts or to improve the scars. In the case of a unilateral procedure, your unaffected breast may need to be adjusted to better match the reconstructed side. This can be accomplished with augmentation, reduction, or lifting of the unaffected breast. This balancing procedure can be done at the same time as the reconstruction or at a second stage operation some months later.
The transfer of fat from one area of the body to the breast area is becoming exceedingly more common. Fat grafting is performed by harvesting the necessary fat using standard liposuction techniques. The fat is then prepared for re-injection and placed where needed through a narrow injection cannula (no additional surgical incisions are made). Fat grafting can be used to improve breast reconstruction in many ways. Fat can provide healthy cells to rejuvenate damaged skin, it can be used to provide additional thickness to thin skin over implants, and it can be used to fill in or correct divots or deformities. These procedures can be done at the same time as the main reconstruction and/or during revision or “touch up” procedures.
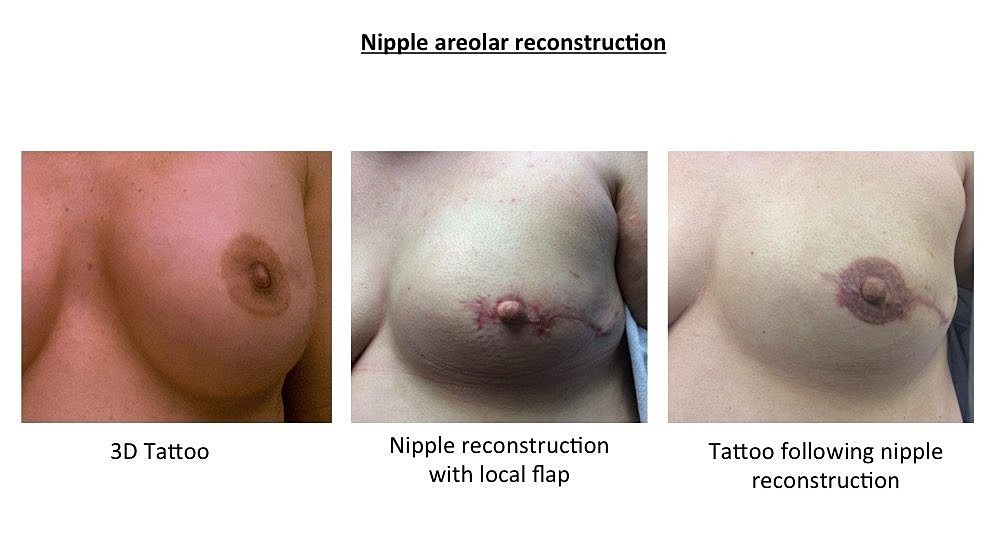
Nipple and areolar reconstruction are optional procedures usually discussed at a minimum of 3 months after final reconstruction of the breast mound. Many options are available to create the colour and appearance of a nipple/areolar complex. Options range from simple tattoo to 3D tattoo reconstruction. If true nipple projection is desired, this can be provided by creating and folding flaps of adjacent breast skin into the shape of a nipple. Alternatively, a graft can be taken from the contralateral nipple (if available) or from other areas such as the earlobe. Nipple/areolar reconstruction is generally performed under local anesthetic with minimal discomfort and recovery time.
Personal factors including your body shape and treatment plan (especially radiotherapy) will impact the options available to you for breast reconstruction. It is important to understand the advantages and disadvantages of a surgical procedure before proceeding with reconstruction.
In general, implant based reconstruction provides a beautiful result with no donor site concerns, a shorter surgery and a faster recovery. In unilateral cases (reconstruction of one breast only), it is often hard to match an implant to a ‘normal’ contralateral breast. Finally, implants are not truly permanent and will likely require smaller revision surgeries in the future. Tissue based reconstructions (abdominal flaps, latissimus dorsi flap) can provide for a beautiful, natural looking breast which can be more easily matched to your contralateral ‘normal’ breast. Since your own tissues are used, they will age and change naturally with the rest of your body and rarely require additional surgery in the future. This comes at the expense of longer surgery and recovery time, as well as significant potential complications at the donor site. Finally, not all women have enough of their own extra tissue from which to reconstruct a breast.
The decision to proceed with breast reconstruction is a personal one. It is important that you are comfortable with your decision. During a consultation with your surgeon, you will discuss all the considerations, including your breast size, breast disease, body shape, other health concerns, lifestyle habits, fears, and goals. Of course, you will also have a detailed discussion of the risks and benefits of the procedures that are right for you. Your surgeon will spend as long as necessary with you to ensure that you understand the options and are ultimately confident in your decision.


